
Page 709 - The Central Motor Vehicles Rules, 1989
P. 709
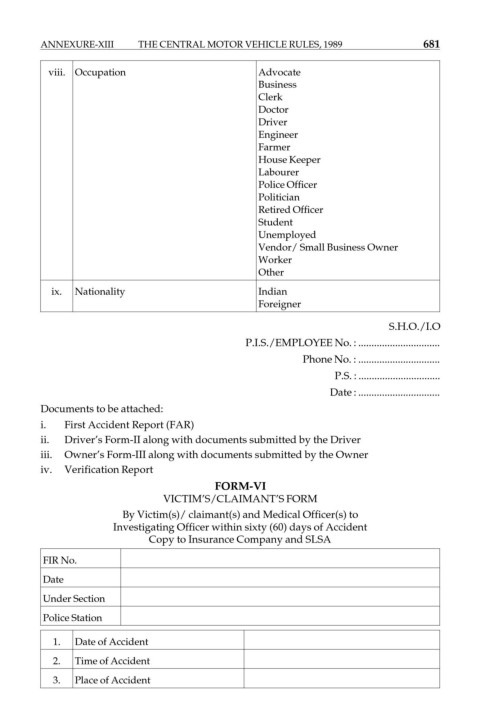
ANNEXURE-XIII THE CENTRAL MOTOR VEHICLE RULES, 1989 681
viii. Occupation Advocate
Business
Clerk
Doctor
Driver
Engineer
Farmer
House Keeper
Labourer
Police Officer
Politician
Retired Officer
Student
Unemployed
Vendor/ Small Business Owner
Worker
Other
ix. Nationality Indian
Foreigner
S.H.O./I.O
P.I.S./EMPLOYEE No. : ...............................
Phone No. : ...............................
P.S. : ...............................
Date : ...............................
Documents to be attached:
i. First Accident Report (FAR)
ii. Driver’s Form-II along with documents submitted by the Driver
iii. Owner’s Form-III along with documents submitted by the Owner
iv. Verification Report
FORM-VI
VICTIM’S/CLAIMANT’S FORM
By Victim(s)/ claimant(s) and Medical Officer(s) to
Investigating Officer within sixty (60) days of Accident
Copy to Insurance Company and SLSA
FIR No.
Date
Under Section
Police Station
1. Date of Accident
2. Time of Accident
3. Place of Accident