
Page 712 - The Central Motor Vehicles Rules, 1989
P. 712
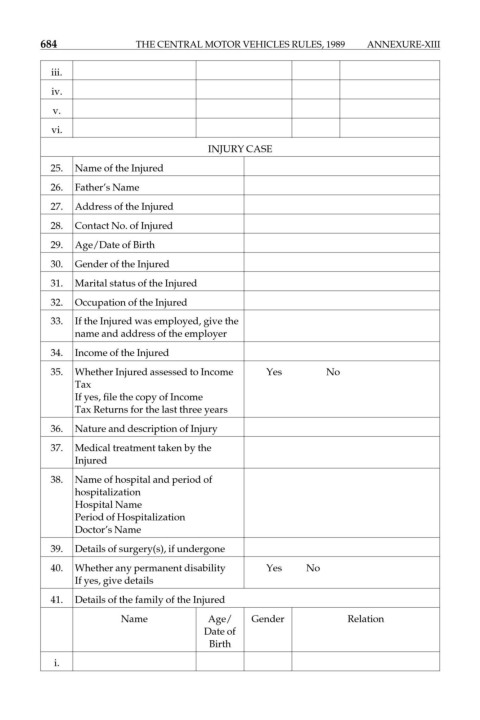
684 THE CENTRAL MOTOR VEHICLES RULES, 1989 ANNEXURE-XIII
iii.
iv.
v.
vi.
INJURY CASE
25. Name of the Injured
26. Father’s Name
27. Address of the Injured
28. Contact No. of Injured
29. Age/Date of Birth
30. Gender of the Injured
31. Marital status of the Injured
32. Occupation of the Injured
33. If the Injured was employed, give the
name and address of the employer
34. Income of the Injured
35. Whether Injured assessed to Income Yes No
Tax
If yes, file the copy of Income
Tax Returns for the last three years
36. Nature and description of Injury
37. Medical treatment taken by the
Injured
38. Name of hospital and period of
hospitalization
Hospital Name
Period of Hospitalization
Doctor’s Name
39. Details of surgery(s), if undergone
40. Whether any permanent disability Yes No
If yes, give details
41. Details of the family of the Injured
Name Age/ Gender Relation
Date of
Birth
i.